
Surgical Oncology
Surgical Oncology is a specialized field within the broader discipline of oncology that focuses on the surgical management of cancer. It plays a crucial role in the comprehensive approach to cancer treatment, working in conjunction with other modalities such as medical oncology and radiation oncology. This branch of oncology aims to diagnose, stage, and treat cancer through surgical interventions
Scope of Surgical Oncology:
Surgical Oncologists are highly trained surgeons with specialized expertise in the management of cancer. Their primary goal is to remove tumors and cancerous tissues while preserving as much healthy tissue and function as possible. Surgical procedures may be used for various purposes, including surgical removal of cancer, performing biopsy to confirm diagnosis and start cancer directed treatment, staging procedures to confirm the exact stage of cancer, and palliative procedures to provide relief from cancer related symptoms in advanced cancers. The scope of Surgical Oncology encompasses a wide range of cancers, including those affecting the breast, lung, gastrointestinal tract, genitourinary system, head and neck, gynaecology and more, however the organ specific approach in surgical oncology offers precision and excellence in cancer care.
Key Procedures in Surgical Oncology:
1. Tumor Resection:
Surgical Oncologists perform radical tumor resections to remove cancerous masses. It is pertinent to remove the cancerous tissue with margins of normal tissue for an adequate surgery which is oncologically safe.The extent of the resection depends on factors such as the type and stage of cancer, as well as the overall health of the patient. These all are major & complex surgeries and better outcomes are expected in hands of well trained and experienced surgical oncologists
2. Biopsy:
Biopsies involve the removal of a small sample of tissue for diagnostic purposes. This helps determine the type of cancer, its stage, and guides further treatment decisions.
3. Lymph Node Dissection:
Many cancers spread to nearby lymph nodes. Lymph node dissection is an important component of performing oncologically safe cancer surgeries. Surgical Oncologists are specially trained in performing lymph node dissection to remove affected nodes, aiding in both staging and treatment.
4. Reconstructive Surgery:
After tumor removal, reconstructive surgery may be necessary to restore the appearance and function of the affected area. This is common in breast cancer and head and neck cancer cases.
Advancements in Surgical Oncology:
1. Robotic aided Surgery:
Minimally invasive surgical techniques such as laparoscopy and robotic-assisted surgery have revolutionized Surgical Oncology, allowing for smaller incisions, reduced recovery times, and fewer complications.
2. Cytoreductive Surgery (CRS) and Hyperthermic Intraperitoneal Chemotherapy (HIPEC) surgery:
Used in advanced abdominal cancers like ovarian, colorectal & stomach cancer with peritoneal disease, peritoneal surface malignancies like pseudomyxoma peritonei (PMP) which have dismal outcomes with conventional treatments. CRS HIPEC is an extensive surgical procedure involving removing all visible disease from the abdomen followed by the delivery of heated chemotherapy directly into the abdominal cavity to kill any remaining cancer cells.
3. Sentinel Lymph Node Biopsy:
This technique helps identify the first lymph node(s) that cancer is likely to spread to, allowing for targeted removal and reducing the need for extensive lymph node dissections. This is particularly useful in early breast cancer, gynaecology cancers & urology cancers.
4. Fluorescence-guided cancer surgeries:
This technology uses the fluorescence imaging which enables the surgeons to identify subtle or hidden tumors, assess the extent of tumor margins, and precisely remove cancerous tissue with minimal impact on surrounding healthy cells. This is particularly useful in colorectal cancers ,breast cancer, gynaecology cancers and urooncology.
Role of Surgical Oncology in Cancer Care:
1. Multidisciplinary Approach:
Surgical Oncology works closely with medical oncologists, radiation oncologists, pathologists, and other specialists to ensure a comprehensive and coordinated tumour board approach to cancer care.
2. Curative and Palliative Care:
Surgical procedures may aim to cure cancer or provide palliative relief by alleviating symptoms and improving quality of life, especially in advanced cases.
3. Postoperative Care:
Surgical Oncologists are involved in postoperative care, monitoring patients for complications and collaborating with other healthcare professionals for adjuvant therapies.
Conclusion:
Surgical Oncology is a dynamic and evolving field at the forefront of cancer care. Through a combination of traditional surgical techniques and cutting-edge advancements, Surgical Oncologists play a pivotal role in the diagnosis, treatment, and management of various cancers. Organ specific oncosurgery programme improves excellence in surgical care and should be adopted. The multidisciplinary approach, coupled with advances in surgical oncology such as robotic aided surgery continues to improve outcomes for cancer patients, offering hope and a path towards a better quality of life.
Gastrointestinal (GI) Cancers
GI cancers arise from the digestive system and include organs like the food pipe (esophagus), stomach, gall bladder, bile duct, liver, pancreas, small intestine (duodenum, jejunum, ileum) and large intestines (colon and rectum).
Symptoms of GI Cancers
Signs and symptoms can vary depending on the location of the cancer within the digestive tract. Some common symptoms include:
- Difficulty swallowing food
- Blood in sputum
- Blood in vomit / brown colored vomiting
- Repeated vomiting
- Repeated heartburn / dyspepsia
- Unexplained weight loss
- Generalized weakness / Unexplained low Hb
- Early satiety / fullness after eating
- Jaundice / yellowish discoloration of eyes
- Change in stool habits - frequency or consistency of stools
- Blood in stools / black colored stools
- Swelling / Distension of abdomen
- Unable to pass stools /flatus
- Any lump in abdome
If you experience any of these symptoms, consult a GI cancer expert as soon as possible.
Diagnosis and Treatment of GI Cancers
Diagnosis typically involves discussing your symptoms, a physical examination, and various tests. These tests help determine the type and extent of the cancer. Some common tests include:
- Blood tests
- Endoscopy or colonoscopy
- Imaging tests (CT scan, MRI, or PET scan)
- Tissue biopsy
Treatment options for GI cancers include surgery, chemotherapy, and radiotherapy. Often, a combination of these treatments is used. A team of specialists, including a GI surgical oncologist, medical oncologist, radiation oncologist, radiologist, and pathologist, will work together to decide the best treatment plan for you.
Keyhole Surgery for GI Cancers
Laparoscopic and robotic surgeries (keyhole surgeries) are performed with good outcomes for GI cancers when done by a qualified and experienced cancer surgeon. These minimally invasive surgeries offer several advantages over traditional open surgery, including:
- Less pain
- Smaller scars on abdomen
- Earlier return to normal activities
- Improved vision, reach, and instrumentation for pelvic surgeries, leading to potentially better outcomes
Advantages of Robotic Surgery
Robotic surgery offers distinct advantages, particularly for pelvic surgeries like rectal cancer. The latest robotic systems provide:
- Improved surgical precision with wristed instruments and 3D visualization
- The possibility of preserving the anal sphincter (avoiding a permanent stoma bag) in select cases
- Potential for better postoperative urinary and sexual function by preserving pelvic nerves
Pancreas Cancer Surgery
Pancreas cancer surgery is a critical intervention aimed at removing cancerous tissues from the pancreas. This complex surgery plays a vital role in treating pancreatic cancer, which is known for its aggressive nature and challenging prognosis. Let's delve into what pancreas cancer surgery entails, the diagnostic investigations involved, the feasibility of keyhole surgery, and the benefits of undergoing such a procedure.
What is Pancreas Cancer Surgery?
Pancreas cancer surgery involves the removal of cancerous portions of the pancreas and, in some cases, surrounding tissues and organs. The primary goal is to eradicate the tumor, alleviate symptoms, and improve survival chances. The two main types of pancreas cancer surgery are:
Whipple Procedure (Pancreaticoduodenectomy):
This is the most common surgery for pancreatic cancer. It involves removing the head of the pancreas, part of the small intestine (duodenum), the gallbladder, and sometimes a portion of the stomach. The remaining sections of the pancreas, stomach, and intestines are then reconnected to allow for normal digestion
Distal Pancreatectomy:
This surgery removes the body and tail of the pancreas and is often performed when the cancer is located in these areas. It may also involve the removal of the spleen.
What Investigations Will Be Done to Diagnose and Treat Pancreas Cancer?
Accurate diagnosis and staging of pancreatic cancer are crucial for effective treatment planning. The following investigations are typically performed:.
Imaging Studies:
CT Scan (Computed Tomography): Provides detailed cross-sectional images of the pancreas and surrounding organs to determine the extent of the cancer.
MRI (Magnetic Resonance Imaging): Offers detailed images and is particularly useful for assessing soft tissues.
PET Scan (Positron Emission Tomography): Helps in detecting cancer spread by highlighting areas of high metabolic activity.
Endoscopic Procedures:
Endoscopic Ultrasound (EUS): Combines endoscopy and ultrasound to obtain detailed images and allows for fine-needle aspiration (FNA) biopsy to collect tissue samples.
ERCP (Endoscopic Retrograde Cholangiopancreatography): Used to visualize the pancreatic ducts and bile ducts, and can also help place stents if there is a blockage.
Blood Tests:
Tumor Markers: CA 19-9 is a common marker that may be elevated in pancreatic cancer, although it is not specific and can be elevated in other conditions as well.
What are the Advantages of Pancreas Cancer Surgery?
Potential for Cure For early-stage pancreatic cancer, surgery offers the best chance for a cure. Removing the tumor completely can lead to long-term survival.
Improved Survival Rates: Combining surgery with other treatments like chemotherapy and radiation can enhance overall survival rates, even in advanced cases
Staging and Planning: Surgical intervention allows for direct assessment and removal of affected tissues, aiding in more accurate staging and subsequent treatment planning.
Conclusion:
In conclusion, pancreas cancer surgery is a pivotal treatment option that can significantly impact patient outcomes. While the journey through diagnosis, treatment, and recovery is challenging, advancements in surgical techniques and comprehensive care approaches are continually improving the prospects for those battling pancreatic cancer.
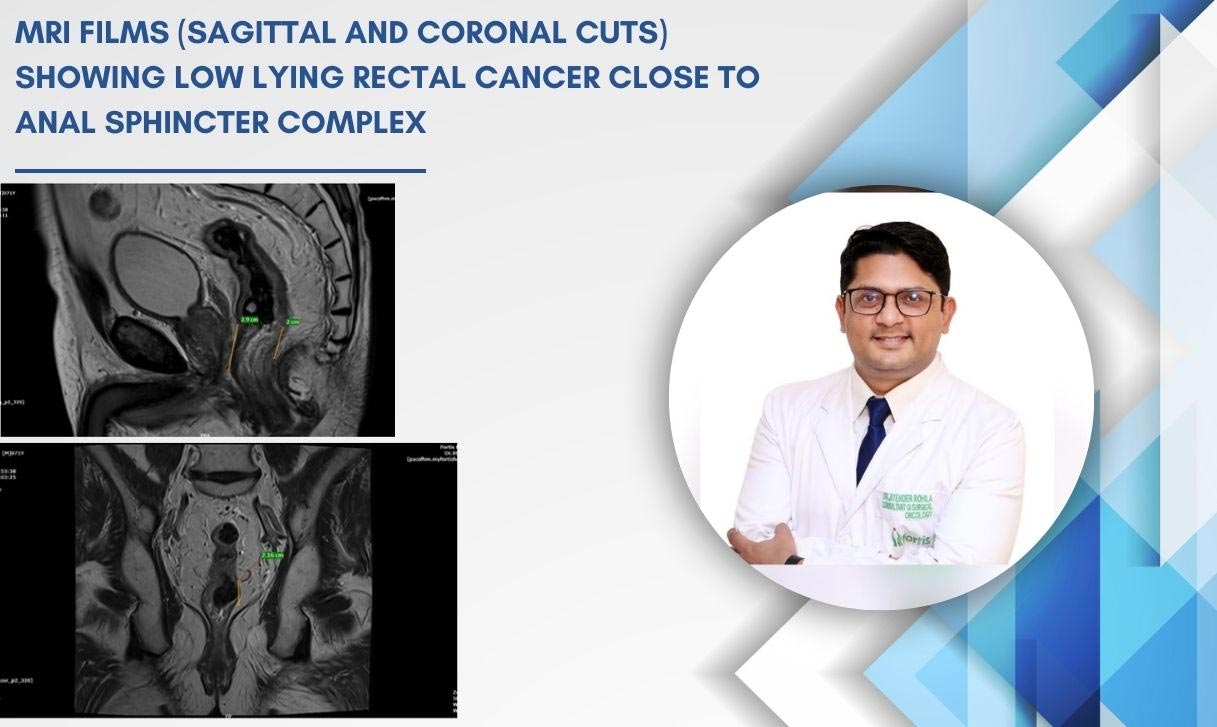
Robotic Sphincter
Saving Surgery for low lying rectal cancer avoiding permanent stoma bag
- 71-year-old male patient presented with bleeding per rectum, changes in bowel habits and loss of appetite since last 3 months.
- On investigations further with Colonoscopy, MRI scan and PET Scan he was diagnosed to have stage 3 low lying locally advanced rectal cancer. Biopsy was Adenocarcinoma.
- He was started with combined radiation therapy and chemotherapy (NACTRT) to shrink the tumor and make feasible for sphincter saving surgery.
- He was reassessed with MRI scan and planned for surgery 6 weeks after completing NACTRT.
Objectively optimize strategic technology without 2.0 bandwidth. Monotonectally administrate user-centric results whereas performance based manufactured products. Continually restore premier strategic theme areas through magnetic customer service. Holisticly embrace optimal processes without B2C infomediaries. Holisticly deploy future-proof leadership skills rather than vertical technologies.
Treatment:
Following discussions with the Tumour Board, there was a good response to NACTRT and Robotic sphincter saving surgery (Ultra Low Anterior Resection) was planned for the patient.
It was a complex surgery which included rectal cancer removal (Total Mesorectal Excision – TME) ensuring tumor free distal margin with removal of the local lymph nodes. The surgery took around 6 hours. After the tumor was removed, ends of large intestine and anal canal were joined (anastomosis) avoiding permanent stoma bag.
The Patient had a smooth post-operative recovery, started walking on Day 1 of surgery, resumed oral feeds on Day 2 and was discharged 5 days after the surgery on 3rd March this year. He has completed his adjuvant chemotherapy and is leading a normal life today.
Discussion on the treatment:
Low lying Rectal cancer (within 5 cm from anal verge) surgery is challenging owing to its location within the pelvis especially in males/high BMI patients and relation to adjacent important structures including anal sphincter which controls the passing of stools. The case attains significance as rectal cancer is one of the commonest GI cancers in the country and permanent stoma bag after surgery is a major concern for majority of patients.
Keyhole surgeries (laparoscopic and robotic) have been used extensively in rectal cancer (large intestine) surgeries worldwide. The general advantage of these surgeries as compared to open surgery include lesser pain, small scars on abdomen and early resumption of normal activities.
The latest Robotic surgery systems (Da Vinci Xi) can improve surgical precision using wristed instruments with seven degrees of freedom (wrist like movement) and a stable three-dimensional (3D) better vision for the surgeon to perform rectal cancer surgeries and allows us to preserve the anal sphincter (avoiding permanent stoma bag); preserve nerves which supply the urogenital organs which can allow these patients to have a good urinary and sexual function after surgery.
Sphincter Surgery
Sphincter surgery, typically referred to as anal sphincter surgery or anal sphincteroplasty, is a procedure performed to repair or reconstruct the muscles of the anal sphincter. The anal sphincter is a group of muscles that control the opening and closing of the anus, facilitating bowel movements and maintaining continence.
Symptoms of Sphincter Surgery
- Fecal Incontinence: Inability to control bowel movements, leading to involuntary leakage of feces.
- Anal Pain or Discomfort: Chronic pain or discomfort in the anal region, especially during bowel movements.
- Difficulty Controlling Gas: Inability to control the passage of gas, leading to embarrassing situations.
- Incomplete Emptying of Bowels: Difficulty completely evacuating the bowels during bowel movements.
- Constipation or Diarrhea: Alterations in bowel habits, which may accompany sphincter dysfunction.
Diagnosis
- Physical Examination: The doctor may perform a physical examination of the anal region to assess sphincter tone and integrity.
- Anorectal Manometry: This test measures the pressure within the anal canal and helps evaluate sphincter function.
- Anal Electromyography (EMG): EMG assesses the electrical activity of the anal sphincter muscles, aiding in diagnosing muscle damage or dysfunction.
- Defecography: A specialized X-ray examination that evaluates the anatomy and function of the rectum and anal canal during defecation.
- Endoanal Ultrasound: This imaging technique helps visualize the internal structures of the anal canal and assess sphincter integrity.
Treatment
The choice of treatment depends on various factors, including the severity of symptoms, underlying causes, and individual patient preferences.
- Conservative Measures: Depending on the severity of symptoms, conservative treatments such as dietary modifications, pelvic floor exercises, and medications may be attempted initially.
- Sphincter Repair Surgery: In cases where conservative measures are ineffective, sphincteroplasty may be recommended. During this procedure, the damaged or weakened muscles of the anal sphincter are repaired or reconstructed.
- Keyhole Surgery (Laparoscopic or Robotic): Keyhole surgery offers benefits such as reduced postoperative pain, shorter hospital stays, and quicker recovery compared to traditional open surgery.
- Biofeedback Therapy: This specialized therapy helps train the pelvic floor muscles to improve bowel control and sphincter function.
- Sacral Nerve Stimulation: In cases of severe fecal incontinence, sacral nerve stimulation may be considered. This involves implanting a device that stimulates the nerves controlling bowel function, helping to improve continence.
If you are experiencing symptoms of sphincter dysfunction, it's essential to consult a healthcare professional for proper evaluation and management.
HIPEC Surgeon
HIPEC Surgery: New-age treatment for abdominal cancers
Chemotherapy is a common cancer treatment and involves administration of medicines or drugs into the body to destroy the fast-growing cancerous cells. The most advanced surgery to treat cancers in the abdomen is through the Hyperthermic Intraperitoneal Chemotherapy (HIPEC), which has revolutionised the treatment of stomach cancer.
What is HIPEC?
HIPEC is administration of heated chemotherapy in the abdomen through a special machine. This stops the spread of cancer cells in the inner lining of the abdomen called peritoneum – a membrane in the abdominal cavity that connects internal organs.
What type of cancers can be treated with HIPEC?
HIPEC is used to treat cancers which have spread to the peritoneum from the appendix, large intestine (colon & rectum), stomach, ovary or cancers that develop from the peritoneum such as pseudomyxoma peritonei, malignant peritoneal mesothelioma and primary peritoneal cancers.
What is the procedure?
HIPEC surgery is a two-stage procedure. The first includes Cytoreductive Surgery (CRS), which is a major surgical procedure wherein the surgeon removes all visible infections from the peritoneum. The second one is HIPEC which involves administration of heated chemotherapy into the abdomen using a specialised HIPEC machine with strict temperature control. After HIPEC is over, chemotherapy drugs are evacuated and the surgeon closes the incisions.
What are the benefits?
The success of a HIPEC surgery depends on several factors such as stage and type of cancer, patient’s age, overall health and performance status etc. It also depends on the quality of cytoreduction surgery done by an expert surgeon in order to achieve the maximum benefit from HIPEC. The best results are seen in PMP (Pseudomyxoma Peritonei) and Peritoneal Mesothelioma. PMP examination has shown a survival rate of more than 10 years with a well-performed complete CRS and HIPEC. CRS HIPEC has also shown good results in a few patients with gastric cancer, colorectal and ovarian cancer.
What is the recovery time?
CRS HIPEC is a major surgical procedure and most of the patients are hospitalised for around 12-14 days. During the stay, the recovery process is monitored closely to detect any complications. The common complications associated with HIPEC are respiratory, renal, chemotherapy-related, incomplete healing of bowel anastomosis and infections. To reduce these complications, it is advisable to consider HIPEC only at tertiary care hospitals which includes surgeons trained in performing HIPEC, trained teams in anaesthesia, ICU critical care, and medical oncology to manage chemotherapy-related complications, expert radiology and oncopathology teams for correct diagnosis (stage, grade and type of cancer), intervention radiology to help manage post-operative complications, and a rehabilitation team to ensure smooth and early recovery.
Thoracic oncologist
Thoracic oncology including - Lung cancer surgery and Mediastinal mass surgery

Chemotherapy is a common cancer treatment and involves administration of medicines or drugs into the body to destroy the fast-growing cancerous cells. The most advanced surgery to treat cancers in the abdomen is through the Hyperthermic Intraperitoneal Chemotherapy (HIPEC), which has revolutionised the treatment of stomach cancer.
What is HIPEC?
HIPEC is administration of heated chemotherapy in the abdomen through a special machine. This stops the spread of cancer cells in the inner lining of the abdomen called peritoneum – a membrane in the abdominal cavity that connects internal organs.
What type of cancers can be treated with HIPEC?
HIPEC is used to treat cancers which have spread to the peritoneum from the appendix, large intestine (colon & rectum), stomach, ovary or cancers that develop from the peritoneum such as pseudomyxoma peritonei, malignant peritoneal mesothelioma and primary peritoneal cancers.
What is the procedure?
HIPEC surgery is a two-stage procedure. The first includes Cytoreductive Surgery (CRS), which is a major surgical procedure wherein the surgeon removes all visible infections from the peritoneum. The second one is HIPEC which involves administration of heated chemotherapy into the abdomen using a specialised HIPEC machine with strict temperature control. After HIPEC is over, chemotherapy drugs are evacuated and the surgeon closes the incisions.
What are the benefits?
The success of a HIPEC surgery depends on several factors such as stage and type of cancer, patient’s age, overall health and performance status etc. It also depends on the quality of cytoreduction surgery done by an expert surgeon in order to achieve the maximum benefit from HIPEC. The best results are seen in PMP (Pseudomyxoma Peritonei) and Peritoneal Mesothelioma. PMP examination has shown a survival rate of more than 10 years with a well-performed complete CRS and HIPEC. CRS HIPEC has also shown good results in a few patients with gastric cancer, colorectal and ovarian cancer.
What is the recovery time?
CRS HIPEC is a major surgical procedure and most of the patients are hospitalised for around 12-14 days. During the stay, the recovery process is monitored closely to detect any complications. The common complications associated with HIPEC are respiratory, renal, chemotherapy-related, incomplete healing of bowel anastomosis and infections. To reduce these complications, it is advisable to consider HIPEC only at tertiary care hospitals which includes surgeons trained in performing HIPEC, trained teams in anaesthesia, ICU critical care, and medical oncology to manage chemotherapy-related complications, expert radiology and oncopathology teams for correct diagnosis (stage, grade and type of cancer), intervention radiology to help manage post-operative complications, and a rehabilitation team to ensure smooth and early recovery.
PIPAC Surgery
Thoracic oncology including - Lung cancer surgery and Mediastinal mass surgery
Expertise in Pressurized Intraperitoneal Aerosol Chemotherapy (PIPAC) for advanced peritoneal cancers, delivering chemotherapy directly to the abdomen minimally invasively, enhancing drug efficacy while reducing systemic side effects.
What is HIPEC?
HIPEC is administration of heated chemotherapy in the abdomen through a special machine. This stops the spread of cancer cells in the inner lining of the abdomen called peritoneum – a membrane in the abdominal cavity that connects internal organs.
What type of cancers can be treated with HIPEC?
HIPEC is used to treat cancers which have spread to the peritoneum from the appendix, large intestine (colon & rectum), stomach, ovary or cancers that develop from the peritoneum such as pseudomyxoma peritonei, malignant peritoneal mesothelioma and primary peritoneal cancers.
What is the procedure?
HIPEC surgery is a two-stage procedure. The first includes Cytoreductive Surgery (CRS), which is a major surgical procedure wherein the surgeon removes all visible infections from the peritoneum. The second one is HIPEC which involves administration of heated chemotherapy into the abdomen using a specialised HIPEC machine with strict temperature control. After HIPEC is over, chemotherapy drugs are evacuated and the surgeon closes the incisions.
What are the benefits?
The success of a HIPEC surgery depends on several factors such as stage and type of cancer, patient’s age, overall health and performance status etc. It also depends on the quality of cytoreduction surgery done by an expert surgeon in order to achieve the maximum benefit from HIPEC. The best results are seen in PMP (Pseudomyxoma Peritonei) and Peritoneal Mesothelioma. PMP examination has shown a survival rate of more than 10 years with a well-performed complete CRS and HIPEC. CRS HIPEC has also shown good results in a few patients with gastric cancer, colorectal and ovarian cancer.
What is the recovery time?
CRS HIPEC is a major surgical procedure and most of the patients are hospitalised for around 12-14 days. During the stay, the recovery process is monitored closely to detect any complications. The common complications associated with HIPEC are respiratory, renal, chemotherapy-related, incomplete healing of bowel anastomosis and infections. To reduce these complications, it is advisable to consider HIPEC only at tertiary care hospitals which includes surgeons trained in performing HIPEC, trained teams in anaesthesia, ICU critical care, and medical oncology to manage chemotherapy-related complications, expert radiology and oncopathology teams for correct diagnosis (stage, grade and type of cancer), intervention radiology to help manage post-operative complications, and a rehabilitation team to ensure smooth and early recovery.